Prevalence= 9/1000 Live birth
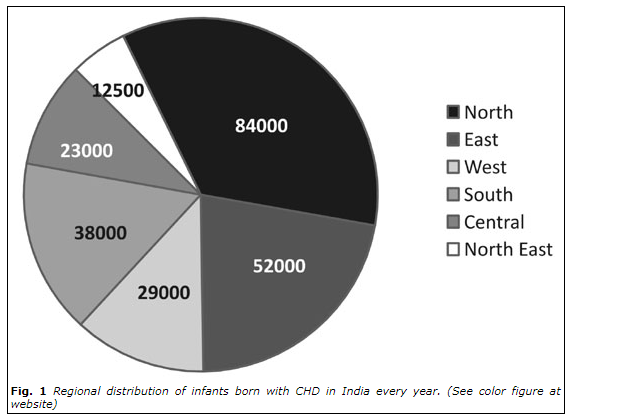
Estimated children born with CHD= 2 lacs, 40 thousands per year
1/5th born to have serious defect- 50000 per year requiring intervention in 1st year
Regional Variation
When should anyone suspect?
Neonates (0-1 month):
Suspect CHD in children if you notice any of the following:
Neonates (0-1 month):
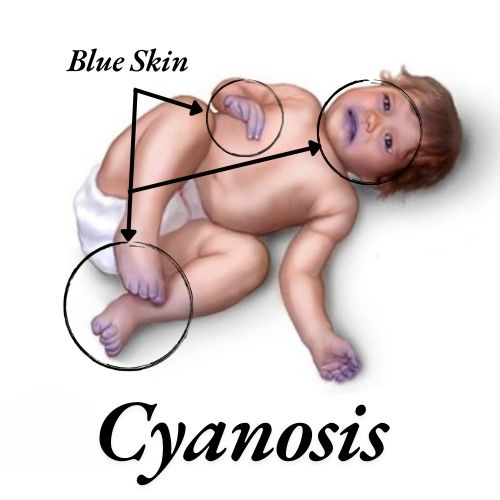
1. Cyanosis (bluish discoloration of skin and mucous membranes)
2. Respiratory distress (rapid breathing, grunting, or retracting)
3. Poor feeding or failure to gain weight
4. Lethargy or irritability
5. Murmur detected during physical examination
When should anyone suspect?
Infants (1-12 months):
Suspect CHD in children if you notice any of the following:
1. Failure to thrive or poor weight gain
2. Recurrent respiratory infections
3. Sweating or pale skin while feeding
4. Fast or difficult breathing
5. Delayed development of milestones
When should anyone suspect?
Children (1-18 years):
Suspect CHD in children if you notice any of the following:
1. Shortness of breath or fatigue during exercise
2. Chest pain or palpitations
3. Dizziness or fainting spells
4. Swelling in legs, ankles, or feet
5. Murmur detected during physical examination
Physical Examination Findings:
1. Abnormal heart sounds or murmurs
2. Clubbing of fingers (enlarged fingertips)
3. Increased heart rate or blood pressure
4. Poor peripheral pulses
5. Hepatomegaly (enlarged liver)
Risk Factors
1. Family history of CHD
2. Maternal diabetes or rubella during pregnancy
3. Premature birth
4. Low birth weight
5. Genetic syndromes (e.g., Down syndrome)
1. Severe cyanosis or respiratory distress
2. Cardiac arrest or shock
3. Sudden collapse or loss of consciousness
4. Severe chest pain or palpitations
Consult a pediatrician or pediatric cardiologist
if you suspect CHD or notice any of these signs or symptoms.
Recommended Screening Schedule:
1. Newborn screening (pulse oximetry) within 24 hours of birth
2. Infant screening (physical examination and history) at 1-2 weeks, 2-3 months, and 6-12 months
3. Child screening (physical examination and history) annually
Early detection and treatment of CHD can significantly improve outcomes and quality of life for affected children.
Why my child is suffering from CHD?
There's usually no clear reason why a baby is born with congenital heart disease (CHD), but some factors may increase the risk:
Genetic Factors
Genetic factors-Some types of CHD are linked to abnormalities in the number or structure of chromosomes, or to single gene defects. Genetic syndromes like Marfan syndrome, Smith-Lemli-Opitz syndrome, and Ellis-van Creveld syndrome are associated with a higher risk of heart defects.
Environmental factors
Environmental factors-Some things the mother did or took during pregnancy may increase the risk of CHD, including:
1. Rubella (German measles)
2. Taking certain medicines, like statins or anti-seizure medicines
3. Smoking or drinking alcohol
4. Having poorly controlled diabetes
Multifactorial Inheritance
Multifactorial inheritance-In 85–90% of cases, there's no identifiable cause. This is thought to be due to multifactorial inheritance, which means that a combination of genes from both parents, plus unknown environmental factors, are involved.
Why my child is suffering from CHD?
If your child has Congenital Heart Disease (CHD), it's essential to work closely with healthcare providers to manage their condition.
Here's a comprehensive guide:
Immediate Steps:
1. Consult a pediatric cardiologist for diagnosis and treatment.
2. Follow recommended treatment plans, medications, and lifestyle modifications.
3. Schedule regular follow-ups with the pediatric cardiologist.
Understanding CHD:
1. Learn about your child's specific heart defect.
2. Understand the treatment options (surgery, catheterization, medication).
3. Recognize potential complications and signs of distress.
Lifestyle Modifications:
1. Nutrition: Ensure a balanced diet, consult a pediatric nutritionist.
2. Exercise: Encourage age-appropriate physical activity, consult a pediatric cardiologist.
3. Sleep: Establish a regular sleep schedule.
4. Stress management: Support emotional well-being.
Medical Management:
1. Medications: Administer as prescribed, monitor side effects.
2. Regular monitoring: Electrocardiograms (ECGs), echocardiograms, blood tests.
3. Surgical or catheter-based interventions: follow ur pediatric cardiologist
Emotional Support:
1. Connect with support groups (e.g., American Heart Association).
2. Seek counseling for your child and family.
3. Encourage open communication.
Adult heart diseases and congenital heart diseases (CHD) in children
Causes in Adults:
1. Adult heart diseases:
Typically result from acquired conditions, such as: -
1. Atherosclerosis (plaque buildup)
2. Hypertension
3. Diabetes
4. Smoking
5. Obesity
Causes in Children:
2. Congenital heart diseases (CHD):
Present at birth, resulting from: -
1. Genetic mutations
2. Environmental factors during fetal development
3. Infections during pregnancy
Adult heart diseases and congenital heart diseases (CHD) in children
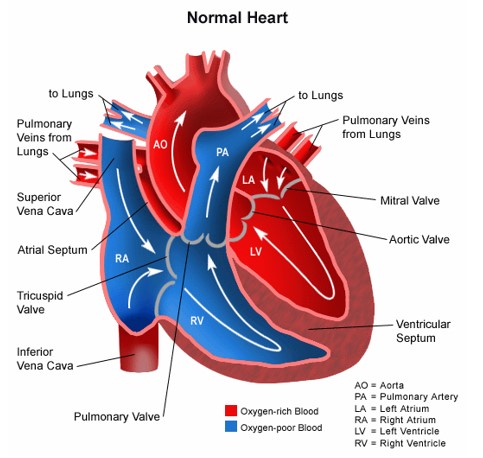
Types of Heart Defects in Children:
1. Atrial septal defects (ASD)
2. Ventricular septal defects (VSD)
3. Tetralogy of Fallot (TOF)
4. Transposition of the great arteries (TGA)
5. Hypoplastic left heart syndrome (HLHS
Adult heart diseases and congenital heart diseases (CHD) in children
Symptoms in Adults:
1. Chest pain or angina
2. Shortness of breath -
3. Fatigue
4. Palpitations
5. Swelling in legs, ankles, or feet
in
Adult heart diseases and congenital heart diseases (CHD) in children
Treatmentin Adults:
A) Adult heart diseases: -
1. Medications (e.g., beta blockers, statins)
2. Angioplasty or stenting
3. Bypass surgery - Heart transplantation
Treatment in Children:
B) Congenital heart diseases (CHD): -
1. Surgical repair or reconstruction
2. Catheter-based interventions
C) Heart transplantation -
1. Lifelong monitoring and follow-up care